Setting: Primary care internal medicine clinic
HPI: Mr. Aaron Turner is a 53-year-old male who presents with fatigue, nausea and vomiting, and leg swelling over the last week. He says the symptoms developed gradually, and now he really can’t eat very much without vomiting. He “just feels terrible” and feels like he has a “sour stomach”. He feels nauseated all the time, whether he eats or not. He denies having any pain.
He has not vomited blood and has not noticed any blood in his urine or bowel movements. He reports he hasn’t been peeing as much as normal. He hasn’t had any abdominal pain or diarrhea, and no one else in his house or at work has been sick that he knows of. His low back has started hurting again after re-starting weightlifting a few weeks ago, so he has been taking some extra doses of naproxen.
PMH:
- Chronic back pain
- Hypertension
Medications:
- Naproxen 500 mg po q 12 hours and prn
- Ibuprofen 200mg PO Q8 hours prn
- Lisinopril 20 mg po daily
- Hydrochlorothiazide 50 mg po daily
Allergies: None
Family History: Heart disease in his father; mother had breast cancer
Social History:
He works as a machinist at the Kentucky Truck Plant. No alcohol, tobacco or illicit drug use.
He has started an exercise routine and is exercising by lifting weights at the gym a few days each week.
Physical Exam
|
Test |
Result |
|---|---|
|
T |
98.1 |
|
HR |
72 |
|
BP |
185/100 |
|
SpO2 |
94% |
|
Weight |
245 lbs (up 30 lbs compared to 3 months ago) |
|
BMI |
30 |
Gen: Ill-appearing but not distressed.
HEENT: + JVD to angle of jaw at 60 degrees elevation. Mucous membranes moist and pink.
CV: S3 heard at lower sternal border, rhythm regular. Pulses strong in all 4 extremities.
Pulm: Rales at the lung bases bilaterally. No dyspnea with ambulating to the exam room or conversation.
Abd: No bruits, no organomegaly appreciated. Bladder not palpable. Bowel sounds present. No pain with palpation. Rectal exam shows normal tone, normal prostate and brown stool.
Ext: 2+ pitting edema to knees bilaterally.
MSK: No muscle tenderness with palpation.
Back: No costovertebral angle tenderness with percussion.
Skin: No lesions noted.
His primary care physician orders a basic metabolic panel and says she will call the patient with the results in a day or two.
These test results return in the evening, and the on-call physician is notified of the following results:
|
Test |
Value |
|---|---|
|
Sodium |
146 mEq/L |
|
Potassium |
6.7 mEq/L |
|
Chloride |
118 mEq/L |
|
Bicarbonate |
16 mEq/L |
|
BUN |
85 mEq/L |
|
Creatinine |
5.1 mg/dL |
|
Glucose |
78 |
The on-call physician checks the patient's electronic health record.
|
Test |
9/9 @ 1445 |
7/9 @ 1400 |
|---|---|---|
|
Sodium |
146 |
145 |
|
Potassium |
6.7 |
4.1 |
|
Chloride |
118 |
119 |
|
Bicarbonate |
16 |
25 |
|
BUN |
85 |
30 |
|
Creatinine |
5.1 |
1.1 |
|
Glucose |
78 |
90 |
She calls the patient and tells him to go straight to the ER. The patient asks if he can just be seen in the morning, but the physician is not comfortable waiting due to the elevation of his potassium and insists he go to the ER immediately. She then phones ahead to the ER to tell the ER physician that the patient is coming in and the reason for referral as well as to report his baseline labs several months prior.
The ER physician sees Mr. Turner after he has been triaged and repeats the physical exam, with no notable changes from the examination performed by the primary care physician earlier in the day.
He orders several additional laboratory tests, an EKG and imaging.
The EKG comes back first:

|
Lab Test |
9/9 @ 2130 |
9/9 @ 1445 |
7/9 @ 1400 |
|---|---|---|---|
|
WBC |
11,000 |
|
|
|
Hgb |
9.1 |
|
|
|
Hct |
27.3 |
|
|
|
Platelets |
331000 |
|
|
|
MCV |
83 |
|
|
|
RDW |
14.1 |
|
|
|
Sodium |
146 |
146 |
145 |
|
Potassium |
7.1 |
6.7 |
4.1 |
|
Chloride |
116 |
118 |
119 |
|
Bicarbonate |
14 |
16 |
25 |
|
BUN |
90 |
85 |
30 |
|
Creatinine |
5.0 |
5.1 |
1.1 |
|
Glucose |
89 |
78 |
90 |
|
ESR |
8 |
|
|
|
CRP |
3 |
|
|
|
C3 |
66 |
|
|
|
C4 |
20 |
|
|
|
BNP |
530 |
|
|
|
Troponin I |
0.061 |
|
|
|
CK |
Normal |
|
|
|
Myoglobin |
Normal |
|
|
|
Urinalysis |
|
|
|
|
Specific gravity |
1.015 |
|
|
|
pH |
6.3 |
|
|
|
color |
yellow |
|
|
|
Protein |
3+ |
|
|
|
Occult blood |
negative |
|
|
|
Nitrate |
negative |
|
|
|
Leukocyte esterase |
negative |
|
|
|
RBC |
0 |
|
|
|
WBC |
0, occasional granular casts seen |
|
|
|
Urine creatinine |
100 mg/dL |
|
|
|
Urine urea |
700 mg/dL |
|
|
|
Urine sodium |
100 mg/dL |
|
|
|
Urine microscopy |
Renal tubular cells and renal tubular cell casts |
|
|
The ER physician places the following orders IV calcium gluconate 6.8 mmol, iv sodium bicarbonate 50mEq, and IV insulin and dextrose, and places the patient on telemetry.
An ultrasound of his kidneys and bladder is ordered. The US demonstrates normal-sized kidneys without hydronephrosis and, as the patient can void without difficulty, a bladder post-void residual is measured and found to be low.
The ER physician then calls the ICU team for admission.
Date: 9/3 @ 0200
The critical care team admits him to the ICU for hypertensive emergency and holds all of his home medications.
Intravenous nicardipine and esmolol infusions are started while nifedipine, isosorbide dinitrate, and hydralazine are titrated for blood pressure control.
During the night, Mr. Turner develops dyspnea and his oxygen saturations drop to 88%. He is placed on oxygen and nephrology and cardiology are consulted. They recommend adding IV furosemide, which is started.
8 hours after the initiation of treatment in the ER, his potassium is 6.0, his BUN and creatinine are 37 and 3.1, respectively and his EKG changes are trending towards normal.
Dates: 9/3 and 9/4
His telemetry continues to be normal.
His input/output is monitored and he has a net negative fluid balance of 2 liters per day.
His intravenous medications are converted to PO.
Selected labs are shown below:
| Lab | Result |
|---|---|
| Sodium | 140 |
| Potassium | 4.8 |
| Chloride | 100 |
| Bicarbonate | 25 |
| BUN | 31 |
| Creatinine | 2.9 |
| Glucose | 85 |
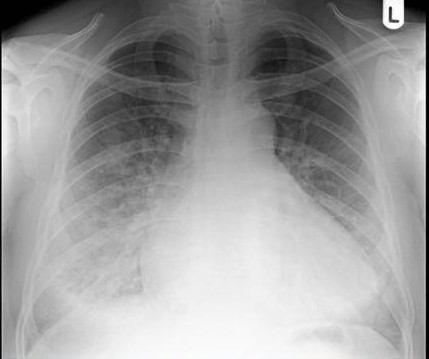
His follow up chest x-ray is shown below:

He is transferred out of the ICU, but will continue to have telemetry monitoring.
Date: 9/5
A 2D echocardiogram shows left ventricular hypertrophy and dilation with a decreased ejection fraction and impaired diastolic function.
The cardiologist tells Mr. Turner that he has a form of heart failure most likely due to his longstanding hypertension.
The nephrologist tells him that he appears to have underlying kidney disease from hypertension and that he got sick because he had a worsening of his kidney function due to multiple factors.
He is advised to receive vaccinations before leaving the hospital and told he will need regular monitoring by his kidney doctor and cardiologist every 3 months for the foreseeable future.
He is discharged on oral nifedipine, hydralazine, isosorbide dinitrate, and furosemide with follow-up in one week with cardiology and nephrology. He is also made an appointment to see a nutritionist and follow up with his primary care physician regarding his desire to resume exercising, lose weight and alternative ways of managing his back pain. For now, acetaminophen is recommended.
